09/2017: A case of abdominal pain, nausea and renal failure
History:
A 15 year old boy presented to the emergency department because of history of abdominal pain and nausea since 6 months. The GP started proton pump inhibitors and anti-emetic medication because of suspicion of his history of autism spectrum disorders and the known frequent gastro-intestinal symptoms in these children. No history of hematuria or dysuria.
BP was 150/86 mm/hg. Laboratory results showed Hb 12.6 g/dl, 9170 10*6/l wbc, 224.000 10*6/l thrombocyte, sedimentation rate 40 mm, CRP 141.5 mg/l. K 5.96 mmol/l, serum bicarbonate 15 mmol/l, Ca 2.68 mmol/l, creatinine 8.08 mg/dl, urea 129 mg/dl, uric acid 14.1 mg/dl. LDH 463 U/l.
Urine test showed no proteinuria (Total protein/creatinine ratio 0.10g/g creat.), No hematuria or pyuria. Culture negative.
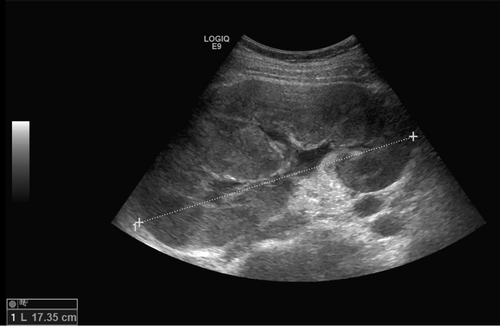
Abdominal ultrasound showed no hepatosplenomegaly but bilateral hyperechogenic kidneys with impressive nephromegaly.
Question:
What is the most likely diagnosis?
- Metabolic storage disease
- Polycystic kidney disease
- Lymphoproliferative disease
- Perlman syndrome
Solution:
Typical history of presentation of renal lymphoproliferative disease is the combination of severe renal impairment with severe hypertensio. However urine sediment was completely normal, without, without hematuria, pyuria nor proteinuria. Ultrasound showed bilateral nephromegaly with increased echogenicity.
Bone marrow and kidney biopsy confirmed the diagnosis of T-ALL. Because of severe renal impairment and the tumor lysis effect after initiation of chemotherapy, the child was dialyszd. Kidney function rapidly improvedment of renal function and kidney size normalized.
Further reading:
Ozaltin F, Yalçin B, Orhan D, Sari N, Caglar M, Besbas N, Bakkaloglu A. An unusual cause of acute renal failure: renal lymphoma. Pediatr Nephrol. 2004;19:912–914
Törnroth T, Heiro M, Marcussen N, Franssila K. Lymphomas diagnosed by percutaneous kidney biopsy. Am J Kidney Dis. 2003;42:960–971